

Infertility is when a couple cannot conceive (get pregnant) despite trying to get pregnant naturally through regular unprotected intercourse. Around one in seven couples may have difficulty conceiving. About 84% of couples will conceive naturally within one year if they have
regular unprotected intercourse.
For every 100 couples trying to conceive naturally:
For couples who have been trying to conceive for more than three years without success, the likelihood of pregnancy occurring naturally (with out any treatment) within the next year is 25% or less.
Some women get pregnant quickly but for others it can take longer. It is a good idea for a couple to visit a fertility specialist if they have not conceived after one year of trying. Women over the age of 35, and anyone who is already aware they may have fertility problems, should see the specialist sooner. The fertility consultant can check for common causes of fertility problems, and suggest treatments that could help.
A couple will only be diagnosed as being infertile if they have not managed to have a baby after one year of trying. There are two types of infertility:
There are many potential causes of infertility and fertility problems can affect either the man or the woman. However, it is not always possible to identify the cause. Common causes of infertility in women include lack of regular monthly release of an egg (ovulation problem), blockage of the fallopian tubes and endometriosis although the cause is unexplained in 25% of couples. In men, the most common cause is poor quality of semen (low sperm concentration, reduced sperm motility, absent sperm). In some men, problem with erection or ejaculation are seen.
Ovulation disorders
Infertility is most commonly caused by problems with ovulation. Some problems stop women releasing eggs at all, and some cause an egg to be released during some cycles, but not others.
Ovulation problems can occur as a result of a number of conditions, listed below.
Tubal problem
The fallopian tubes are the tubes along which an egg travels from the ovary to the womb. The egg is fertilised as it travels down the fallopian tubes. When it reaches the womb, it is implanted into the womb’s lining where it continues to grow. If the womb or the fallopian tubes are damaged, or stop working, it may be difficult to conceive naturally. This can occur following scarring from surgery or previous infection in the pelvis (pelvic inflammatory disease) or endometriosis.
Fibroids
Fibroids in the uterus are benign (non-cancerous) tumours that grow in the uterus. These are very common and are do not usually cause any problem. Depending on its location and size, fertility can be affected. Submucous fibroids (fibroids lying close to the inner lining of the uterus or with in the cavity of uterus) and large intra-mural fibroids (fibroid that are seen with in the muscle of uterus) can reduce fertility, although exactly how they do this is not yet known. It is possible that a fibroid may prevent an embryo from implanting itself into your womb.
Endometriosis
Endometriosis is a condition where lining of the uterus, known as the endometrium, starts growing in other places, such as the ovaries. This can cause infertility because the new growths form adhesions (sticky areas of tissue) or cysts (fluid-filled sacs) that can block or distort the pelvis. These make it difficult for an egg to be released and become implanted into the womb. It can disturb the way that a follicle (fluid-filled space in which an egg develops) matures and releases an egg.
Medicines
The side effects of some types of medication and drugs can affect your fertility.
Age
Infertility in women is also linked to age. The biggest decrease in fertility begins during the mid-thirties.
Abnormal Semen parameters
Some possible reasons for abnormal semen are listed below.
Many cases of abnormal semen are unexplained. The factors that can affect semen and sperm in some men are Infection or trauma of testes or genital area, testicular cancer, surgery to testes or genital area, undescended testes (testes not descened into the scrotum), congential defect (defect from birth) such as absence of vas deference (tube carrying sperm from testes to penis). Smoking and excessive alcohol intake can also affect semen quality.
Erectile or ejaculation problem
Some men experience erectile or ejaculation problem that can make it difficult for them to ejaculate. Other ejaculation problems include retrograde ejaculation (semen is ejaculated into bladder) and premature ejaculation (ejaculation occurs too quickly before entering into the vagina)
Hypogonadism
Rarely, abnormal testicular function or pituitary gland function can be a cause for abnormal sperm production. This could be due to a tumour, taking illegal drugs, or Klinefelter’s syndrome (a rare genetic condition where a man is born with an extra female chromosome).
Medicines and drugs
Certain types of medicines can sometimes cause infertility problems.
There are a number of factors that can affect fertility in both men and women.
Weight
Being overweight or obese reduces both male and female fertility. In women, being overweight can affect ovulation. Being underweight can also have an impact on fertility, particularly for women, who will not ovulate if they are severely underweight.
Smoking
Smoking can adversely affect fertility in addition to its ill effects on general long term health.
Occupational and environmental factors
Exposure to certain pesticides, metals, and solvents can affect fertility in both men and women.
Exposure to heat and working in a hot environment can affect sperm quality.
Stress
Stress can affect relationship as well as fertility. Stress can contribute to a loss of libido (sex drive), which in turn can reduce the frequency of sexual intercourse. Severe stress may also affect female ovulation and limit sperm production.
Fertility testing and investigation can be a lengthy process, and female fertility decreases with age,so it is best to make an appointment early on. It is always best for both partners to visit the fertility unit because fertility problems can affect a man or a woman and sometimes both partners. The process of trying to conceive can be an emotional one, so it is important to support each other as much as possible.
When you visit the specialist, they will want to discuss your full medical, sexual and social history. This will help them identify what may be causing fertility problems.
Age
Fertility in women declines with age, and your GP will discuss this with you.
Previous pregnancy
Your doctor will want to discuss any previous births and any related complications with your pregnancy. They will also ask about any miscarriages you may have had.
Length of time trying to conceive
Your doctor will ask how long you have been trying to conceive. Evidence from studies indicate that the chances of pregnancy following regular unprotected intercourse for women:
Sexual intercourse
You will be asked how often you have intercourse, and whether you have any difficulties during intercourse. You may feel uncomfortable or embarrassed about discussing your sex life with your doctor. However, it is very important to be open and honest. If the fertility problem is to do with sex, it might be overcome easily.
Length of time since stopping contraception
You will be asked about the type of contraception you previously used, and when you stopped using it. It can sometimes take a while for certain types of contraception to stop working, and this may be affecting your fertility.
Medical history and symptoms
Your doctor will want to discuss any medical conditions you have, or have had in the past. For womn, your doctor may ask how regular your periods are and whether you experience any bleeding between periods or after sex.
Medication
The side effects of some medication can affect your fertility. So your doctor will look at any medication you are taking, and might discuss alternative treatments with you. You should mention any non-prescription medication you are taking, including herbal medicines.
Lifestyle
Several lifestyle factors can affect your fertility. Your doctor will want to know on smoking, weight and height (body mass index), alcohol intake, stress levels and any history of illegal drug intake (eg: anabolic steroids). They may recommend changes to your lifestyle to increase your chances of conceiving.
After taking a medical, sexual and social history, your doctor may carry out a physical examination, or refer you directly for investigations. The examination include height and weight to check body mass index (BMI) for both men and women, pelvic examination to check for infection or any tenderness or lumps for women and scrotal examination for men.
For women, a number of tests can be used to try and establish the cause of infertility.
Hormone tests
A sample of your blood can be tested for certain hormones (FSH, LH, prolactin or thyroid stimulating hormone, progesterone) to check for ovulation, egg reserve, pituitary and thyroid function depending on various clinical factors. The timing of the test is depending on the test to be done and also based on how regular your periods are.
Checking your ovaries by ultrasound
Your ovaries may be tested before you are offered fertility drugs. This may be either a blood test to measure certain hormones or an ultrasound scan to examine the follicles in your ovaries.
Tests for infection
A swab (similar to a cotton bud, but smaller, soft and rounded) is used to collect some cells from your cervix to test for infections. If you have infections, you will be prescribed antibiotics to treat it.
Hysterosalpingogram (HSG)
A hysterosalpingogram is a type of X-ray taken of your uterus and fallopian tubes after a special dye has been injected. This will outline the cavity of your womb and detect any blockage of the fallopian tubes (Figure 1 and 2).
You will be advised to take an antibiotic and a pain killer in advance prior to the procedure. You will also need to have protected intercourse (using condom) from the last period until time of the test. Generally the test will be performed soon after the bleeding during period has stopped. During the procedure, a cannula will be passed through the cervix (opening of the uterus). A contrast dye will be injected into the uterus and then an X-Ray will be performed to assess the patency of the tubes. The whole procedure is very quick and takes about 5-10 minutes. You will be able to go home straight after the procedure.
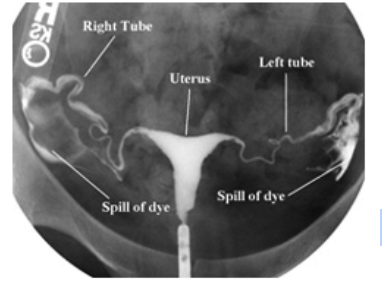
Figure1: HSG demonstrating normal uterine cavity and patent fallopian tube

Figure2: HSG demonstrating blocked fallopian tube with hydrosalpinx (swollen and enlarged tubes)
Hysterosalpingo-contrast-ultrasonography(HyCoSy)
A hysterosalpingo-contrast-ultrasonography is a type of ultrasound scan and is an alternative to HSG to check for any blockage of the fallopian tubes. A small amount of fluid will be injected into your womb through a tube (Figure 3 and videio 1). Ultrasound is used to confirm whether this fluid spills through the tubes.

Figure 3: A catheter is introduced into the uterus to inject the contrast dye
Video 1: This HyCoSy ultrasound scan video is demonstrating patent tubes with dye going through the tube.
Laparoscopy and Dye test
A laparoscopy involves making a small incision (cut) in your lower abdomen. A thin, tubular telescope called a laparoscope will be used to look more closely at your womb, fallopian tubes and ovaries. Dye may be injected into your fallopian tubes through your cervix to highlight any blockages in them. A laparoscopy is usually only used if there is a strong chance that you have a problem – for example, if you have had a history of pelvic infection in the past.
Semen analysis
Semen will be tested to determine whether there is a low sperm count, low sperm mobility, or abnormal sperm
For some couples, general advice on leading a healthy life style and being aware of ‘fertility window’ (the time period when the chances of fertility is maximum) and having regular intercourse during the fertility window would only be sufficient to improve fertility.
Types of specific fertility treatment available include:
The treatment offered will depend on the cause of your fertility problems, women’s age and egg reserve and also duration of infertility. The success rates and risks vary depending on treatment
Medicines are often used to assist fertility. These are usually prescribed for women, although in some cases they may also be prescribed for men.
Surgical procedures that may be used to investigate fertility problems and assist with fertility are listed below.
Surgery may be advised to repair the fallopian tubes if tubes have become blocked or scarred due to previous infection or surgery. Surgery is done to break up the scar tissue or to open up the blocked tubes, making it easier for eggs to pass along them. The success of the surgery will depend on how damaged the fallopian tubes are.
Laparoscopic surgery is often used for women who have endometriosis (when parts of the womb lining start growing outside of the womb), to destroy or remove cysts (fluid-filled sacs). If there are any fibroids laparoscopic or hysteroscopic removal of fibroids (myomectomy) is advised.
In women with PCOS, laparoscopic ovarian diathermy (LOD) may be used in resistant cases where ovulation medication has not worked.
In men with blocked epidydimis or vas (which transport sperm from testes), surgery to correct the blockage may be recommended.
Surgical sperm extraction (SSR) may be an option for men with azoospermia (absent sperm in semen sample). Any material with sperm can be frozen and placed in storage for use at a later stage for IVF/ICSI treatment. If surgical retrieval of sperm is successful, usually enough sperm is obtained for several cycles of treatment (if required).
Intrauterine insemination (IUI) is a procedure that bypasses the cervix and places sperm into a woman’s uterus around the time of ovulation. Placing the sperm directly into the uterus makes the trip to the site of fertilization (fallopian tubes) much shorter. This way, there is a better chance that more sperm will make their way closer to the egg and thereby improving a woman’s chance of getting pregnant. Provided that the man's sperm and the woman's tubes are healthy, the success rate for IUI in women under 35 is around 15% for each cycle of treatment.
While IVF and ICSI have been originally recommended for subfertility associated with tubal problems and sperm problems respectively, these have now become the choice, if all other fertility treatments have proven unsuccessful. IVF is a method of assisted reproduction in which a man’s sperm and a woman’s eggs are combined outside the body in a laboratory dish. One or more fertilized eggs (embryos) can then be transferred into the woman’s uterus, where they may implant in the uterine lining and develop. Excess embryos may be cryopreserved (frozen) for future use. IVF is the recommended treatment to the couples, who experience in delay in conceiving due to factors that prevent the union of sperm and egg (blocked, damaged or absent fallopian tubes). If the subfertility is due to male factor with low sperm count or low sperm motility, the embryologists inject a sperm into the egg manually (Intra-cytoplasmic sperm injection, ICSI) to fertilize the eggs. IVF and ICSI are advised for all other causes of subfertility (endometriosis, ovulation problems or unexplained) also especially if the couple have been trying for a long period of time and other treatments have been unsuccessful. If you or your partner has an infertility problem, you may be able to receive eggs or sperm from a donor to help you conceive. Treatment with donor eggs is usually carried out using IVF. The success rate for a cycle of IVF/ICSI is about 35-40% for women under 35 years of age. The success rate decreases as the woman’s age increases.
Some infertility treatments can cause complications, including side effects from medication and multiple pregnancy.
Some medications used to treat infertility can cause side effects. These may include nausea, vomiting, stomach discomfort, headaches, hot flushes and injection site bruising and pain.
If you have IVF, you have a slightly higher risk of an ectopic pregnancy where the embryo implants in the fallopian tubes rather than in the uterus. If you have a positive pregnancy test, you ll have a scan at six weeks to make sure the embryo is growing properly and that pregnancy is normal. Tell your doctor if you experience vaginal bleeding or tummy pain after having IVF and a positive pregnancy test. Multiple pregnancy If more than one embryo is replaced in the womb as part of IVF treatment, there’s an increased chance of producing twins or triplets. Having more than one baby may not seem like a bad thing, but it significantly increases the risk of complications for you and your babies like miscarriage (abortion), preterm births
If more than one embryo is replaced in the womb as part of IVF treatment, there’s an increased chance of producing twins or triplets. Having more than one baby may not seem like a bad thing,but it significantly increases the risk of complications for you and your babies like miscarriage (abortion), preterm births
